
Diabetes Mellitus is a metabolic disease that induces elevated blood sugar. In order to store or use glucose, the hormone insulin transfers sugar from the blood into cells. With diabetes, the body either does not produce enough insulin or is unable to use the insulin it produces effectively.
Diagnosis of diabetes mellitus is readily known when a patient has classic symptoms of hyperglycemia (high levels of sugar, or glucose) and has a random plasma glucose level of 200 mg/dL or higher.
Type 2 diabetes is by far the most common type of adult diabetes (more than 90 percent) and is characterized by hyperglycemia and varying degrees of insulin resistance and deficiency. Most patients with type 2 diabetes are asymptomatic, and routine laboratory examination indicates hyperglycemia, requiring further study. Polyuria, polydipsia, nocturia, blurred vision, and weight loss are classic hyperglycemic symptoms.
Type 1 diabetes is characterized by autoimmune disruption of the beta cells of the pancreas, resulting in total deficiency of insulin. In approximately 25 percent of adults with newly diagnosed type 1 diabetes, diabetic ketoacidosis (high levels of blood acids called ketones) can be the initial occurrence. The loss of insulin secretory ability in adults with type 1 diabetes is normally less pronounced compared to children, but adults with type 1 diabetes generally have a longer symptomatic duration (polyuria, polydipsia, weight loss, fatigue) prior to diagnosis than children.
Fasting sugar blood tests or A1c blood tests, also referred to as glycated hemoglobin tests, are used to diagnose diabetes. After fasting for at least eight hours, a fasting blood sugar test is performed. Less than 100 mg / dl is normal fasting blood sugar. For an A1c blood test, patients do not have to fast.
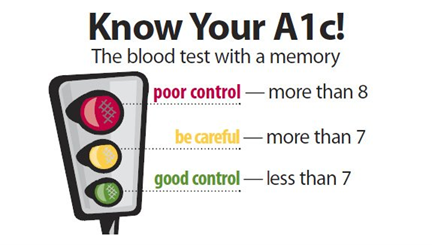
A significant blood test to diagnose diabetes or assess diabetes control is the glycosylated hemoglobin test. It gives an average assessment of blood glucose over the past 3 months and is used to make medication changes in accordance with home glucose monitoring.
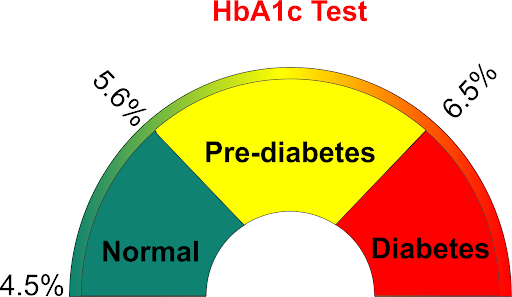
For those without diabetes, the standard range for the A1c test is less than 5.7 percent, 5.7 percent-6.4 percent for those with pre-diabetes. It is 6.5 percent or higher for people with diabetes. Two distinct A1c tests at 6.5 percent are positive for diabetes for diagnostic purposes. This test should be done 4 times a year (every 3 months) by people with diabetes who are treated with insulin. Every 4 to 6 months, those who are not treated with insulin should have this exam.
The diagnosis of diabetes in an asymptomatic individual (generally type 2 diabetes) can be established based on the American Diabetes Association (ADA) criteria.
American Diabetes Association criteria for the diagnosis of diabetes:
- A1C ≥6.5%. The test should be performed in a laboratory using a method that is NGSP certified and standardized to the DCCT assay
- FPG ≥126 mg/dL (7.0 mmol/L). Fasting is defined as no caloric intake for at least 8 hours
- 2-hour plasma glucose ≥200 mg/dL (11.1 mmol/L) during an OGTT. The test should be performed as described by the World Health Organization, using a glucose load containing the equivalent of 75-gram anhydrous glucose dissolved in water
- In a patient with classic symptoms of hyperglycemia or hyperglycemic crisis, a random plasma glucose ≥200 mg/dL
A1C: glycated hemoglobin; NGSP: National Glycohemoglobin Standardization Program; DCCT: Diabetes Control and Complications Trial; FPG: fasting plasma glucose; OGTT: oral glucose tolerance test.
Diagnosis requires two irregular test results from the same sample or two different test samples, in the absence of unequivocal hyperglycemia. The most widely used clinical test to estimate blood glucose control is glycated hemoglobin measurement (also called A1C, hemoglobin A1C, glycohemoglobin, or HbA1C). A1C reflects mean blood glucose for the full 120-day lifespan of the red blood cell. It is used in conjunction with home glucose monitoring to make treatment adjustments.
Individuals almost often have “prediabetes” until they acquire type 2 diabetes. Blood sugar levels are higher than usual but not quite high enough to be classified as diabetes. Doctors also refer to prediabetes as impaired glucose tolerance (IGT) or impaired fasting glucose (IFG), depending on what test was used when it was identified. This condition puts individuals at a higher risk of developing cardiovascular disease and type 2 diabetes. Individuals should be tested, in one to two years for type 2 diabetes if they have prediabetes.
Results indicating prediabetes are:
- An A1C of 5.7%–6.4%
- Fasting blood sugar of 100–125 mg/dl
- An OGTT 2-hour blood sugar of 140 mg/dl–199 mg/dl
Glycated hemoglobin measurement (also called A1C, hemoglobin A1C, glycohemoglobin, or HbA1C) is the most frequently used clinical test to estimate blood glucose regulation. A1C represents mean blood glucose over the red blood cells entire 120-day lifetime, but it is better compared with mean blood glucose over the previous 8 to 12 weeks.
Individuals will not immediately develop type 2 diabetes if they have prediabetes. Early treatment will return blood sugar levels to the normal range for certain individuals with prediabetes. Research shows that you can lower your risk for type 2 diabetes by 58% by losing 7% of your body weight (or 15 pounds if you weigh 200 pounds and exercising moderately (such as brisk walking) 30 minutes a day.
A C-peptide test is often used to help tell the difference between type 1 and type 2 diabetes. With type 1 diabetes, pancreas makes little to no insulin, and little or no C-peptide. With type 2 diabetes, the body makes insulin, but does not use it well. This can cause C-peptide levels to be higher than normal.
In type 1 diabetes, a microalbumin test is recommended once a year beginning five years after the diagnosis. In type 2 diabetes, a microalbumin test is advised once a year beginning immediately after the diagnosis.
If the microalbumin creatinine ratio shows albumin in urine, patients may get tested again to confirm the results. If results continue to show albumin in urine, it may mean early-stage kidney disease. If test results show high levels of albumin, it may indicate kidney failure.
To prevent the complications of diabetes, few pathology investigations are recommended which include renal function tests (Blood Urea Nitrogen (BUN), Serum Creatinine, Albumin test, sodium and potassium levels and Glomerular Filtration Rate). Along with it, urine microalbumin test is advised to detect very small levels of a blood protein (albumin) in the urine. A microalbumin test is used to detect early signs of kidney damage in people who are at risk of developing kidney disease.
In COVID-19, diabetes mellitus (DM) is a recognized risk factor for serious disease and mortality. It is partially due to the defective immune system found in uncontrolled DM patients. The immune system’s innate and adaptive arms are both weakened in DM.
Above all, patients should undergo plasma glucose level and HBA1c test at regular intervals depending upon the severity of diabetes mellitus.
November is the Month of National Diabetes. The priority this year is on taking care of young people who have diabetes. Diabetes is one of the most common chronic conditions in the United States among school-age teenagers, affecting about 193,000 young people under the age of 20. Regardless of their age, young people with diabetes often need assistance with their diabetes treatment. That is why it is important to help young diabetic patients create a diabetes management plan and work to change the diabetes self-care plan when required with their health care team.
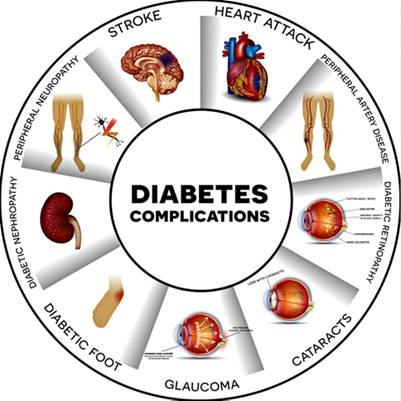
Managing blood glucose levels and making sure that young diabetic patients take their medications as prescribed in the right dosage, at the right time. A balanced eating schedule, adequate sleep, and daily physical activity should be encouraged. Before, during, or after physical exercise, teens with type 1 diabetes should also monitor their blood glucose levels. During a pandemic, face coverings, hand sanitizer, and disinfecting wipes can also be added to the ‘go-kit’. Emphasis is also given to monitor for complications of diabetes. Early diagnosis and treatment will help to minimize the risk of heart disease, loss of vision, nerve damage, and other health issues associated with it. They should also be prompted to seek treatment for mental wellbeing.